Scott and I got together and started talking with intentions of discussing the future of Physical Therapy and possible opportunities that exist now. …maybe we accomplished that, maybe not. But we like talking to each other, and we hope you’ll like listening to us.
I have had a lot of conversations around pay in Physical Therapy over the past couple of years. A pattern has developed that leads me to believe we have been approaching pay the wrong way. We have failed at improving PT insurance pay, but not for any lack of effort. Suddenly, there may be a new opportunity for systemic change that I believe we must take full advantage of. In the last few months, we have seen the COVID pandemic set the stage for large changes in just about every aspect of life – especially in the provision of healthcare.
In physical therapy, we have taken the stance that our services save the system money. When people interact with us, there is less medication use, less imaging, and less surgeries – usually with comparable results. Every time research is conducted on the most common musculoskeletal conditions – i.e. back pain, neck pain, meniscus tear, rotator cuff tears – we get the same results: purely anatomical findings are not as predictive of dysfunction as the medical model thinks. Physical Therapists often get superior results for exponentially less cost. This is the truth, and this has been our consistent talking point to insurers, regulators, and legislators.
Last year, I went to a conference put on by the American Chiropractic Association in conjunction with Physical Therapist and Osteopathic professional groups. One speaker, who was formally trained as a Chiropractor, but working as a higher-up in United Health Care spoke bluntly on the topic of increased insurance payment. He said, plainly, bluntly, and quite rudely, that insurance companies do not care who saves the system money. That is not what they are looking at. He does not care about our value proposition.
That was the first time I considered that our kumbaya approach to saving health care makes a lot of sense to us, but may only be valuable through a therapist’s eyes – not the view of others. This insurance exec went on to say that what UHC is looking for in a valuable professional encounter is one in which the patient doesn’t return. Meaning, they are cured and the insurance company is no longer on the hook for the bill. I’ve been turning this over in my head for more than half a year now, and I still can’t make sense of it. My best guess is people change insurance plans so often that the insurance companies want a short, finite episodes of care that ends in a tangible result (good or bad). They do not want the prolonged liability of someone who may be getting gradually better over several months of rehab, even if waiting to see the outcome of rehab would save billions of dollars over the entire population. It seems like bad math to me, but I digress.
Within a few weeks of the ACA conference, all the PTs, OTs, and SLPs I work with had a meeting with HR at our community hospital. There were some changes being announced in the pay structure at work and HR wanted to present it to us with an opportunity for questions – I assume we were given extra attention because we are notorious for complaining about being underpaid.
The hospital was switching to a market-based pay system. Meaning, our pay would be established by the pay of other hospitals around us. The HR employee told me, point blank, that the money our department brings in has no influence on what our pay is.
After hearing HR tell me the money I make for the hospital has no influence on the money I make for myself, and the insurance executive telling me that my saving him money doesn’t mean I’ll get paid more – I was starting to have doubts about our whole profession’s approach to increasing our insurance payments and overall pay. It seems the factors that we think impact our pay do not. Saving insurers money doesn’t get us paid more. Making our employers money doesn’t get us paid more. We need a new playbook.
At the end of last year, a large group of leaders in the Academy of Orthopaedic Physical Therapy (AOPT – formerly the Ortho Section of APTA) got together to make the strategic plan for the next 6 years. A part of that process was surveying the nearly 20,000 members about their priorities for the Academy’s work – about 300 people replied with information that would ultimately help guide our work.
The survey, though poorly responded, had clear results. Members of AOPT and APTA want leadership working on increasing insurance payment and the value of PT. This was made central to the strategic plan which I encourage you to take a very quick look at: https://www.orthopt.org/uploads/content_files/files/2020%20Strategic%20Framework.pdf
Increasing pay from insurers is work APTA has advocated for daily for years. That Members want increased pay is not new information to anyone. There are annual conferences focusing on payment, groups from all over APTA work constantly in many ways to increase payment, but what do we see? Decreasing reimbursements. Which brings me back to what I have expressed above – what we think should work, does not. Throw. Out. The Playbook.
AOPT will be addressing payment in a more direct way than previously. I hope novel approaches are researched, the who’s-who of payment in rehab are gathered, and the dissenting insurance executives are consulted. There has to be something we can do to increase our insurance payment for our valuable services that cure patients for far less cost than the other more invasive alternatives.
I had one more very recent conversation. I have this patient I’ve seen off-and-on for a couple years. He is a bonafide titan of industry – the real deal. He has held very big positions in businesses you know. The other day, he comes into his appointment talking to me as he often does about whats going on in the world and what might be the next big money-maker/world-changer. But this time, he is suddenly talking my language.
He says there are several major revolutions that will be coming from the COVID-19 pandemic and one of them will be in healthcare. He says we have long assumed that what the DOCTOR (Physician) says is right. That we rely on very tangible procedures for well defined problems to get tangible results – simply, surgery for broken and torn stuff, but that time and conservative measures can get a lot of the same results for far less money. He says people who delayed surgeries during COVID shutdowns are seeing good results in their recoveries without having had the surgeries they previously planned on having. He suggests that part of the revolution will be an investment in value-based treatments that save the system money. He stresses preventative medicine over interventional medicine. This guy isn’t saying the words “Physical Therapy,” but those are the words my ears are hearing.
So what do I think now? Is our old mantra, our kumbaya-ing, on the brink of finally paying off in our society’s most desperate time? Or is it time to move on and see what our new approach should be? I’m really not sure, but if you’re not a payment expert and you’re not working directly in the insurance industry, there is one way for you to directly contribute to and be a part of the effort that finally gets Physical Therapists the financial respect we damn-well deserve. Become a Member of APTA and AOPT – the work is being done at the highest level and may be on the edge of the breakthrough we have all been waiting for. This is your chance to contribute to the cause, and you might be jumping on the bandwagon at exactly the right moment.
Scoot and I are buds from the travel PT days in Aspen. We talk often, it usually digresses in some PT shop talk.
We got on Zoom and talked for over two and a half hours recently. I was able to trim it down to about a 30 min recording. We think we’re hilarious. We think we have good ideas about PT. Give us a try – I think you’ll be entertained and maybe informed too.
If you’re into cable, we’re better than anything on there… and maybe half of Netflix. Play us in the background while you do dishes or something, but try us out. If you like it, we’ll do more in shorter format.
I’m not one of those people who writes, stops, crumples up a ball of paper, and starts over. Usually, I sit down at the computer, write whatever comes to mind and move on with a few edits later. This time, I just can’t get this blog going. I’ve started, stopped, started-over, and re-started over. There’s so many obstacles to writing this blog. The biggest barrier is that while many of us are finding ourselves with additional free time, we are so all-consumed with this virus that we can’t seem to get anything done – like writing this blog. Another huge barrier has been the speed things are moving at, every time I think I have a handle on what’s happening in healthcare and with the virus, it changes. Finally, I think I’ve been trying to fit too many ideas in one blog that truly contradict with each other.
Contradictions, that seems to be the hallmark of this crisis. While some facilities are laying off all their staff from lack of work, others are overloaded and woefully understaffed. One minute I’m convinced we’re all doomed to big, big trouble, the next I know we’ll be fine, then I swing back the other way. Should my last few remaining patients be scared of what I could spread to them, or should I be scared of what they will spread to me? I worry and I’ve had to quickly learn to manage that.
All those contradictions are why this has now become at least 2 separate blogs, maybe more if this isolation drags on. In this first one, I’d like to lay out the challenges that many travelers are facing in this crisis and some of the resources that are out there to help those challenges. In the sequel to this blog, I’d like to take a more positive note and look at some of the opportunities for change this crisis will bring. But I can’t write that piece without first writing this one that expresses the true graveness of this situation.
We’ll see if I get through writing this. Things will undoubtedly change before I can push that “publish” button. So please grant me some grace in knowing that what I write today may be outdated or completely inappropriate by tomorrow.
This thing is moving very fast. A few weeks ago, I was finishing up a paternity leave in Hawaii. The impetus for the trip was the wedding of an old travel PT friend. At that time in the beginning of March, the COVID-19 concern had started to build, but wasn’t doing much to affect every day life. The wedding went off without a hitch, was awesome, and was full of international guests and current/former Travel PTs and OTs from all over the country. I haven’t heard of a single illness from that wedding. Phew.
The next Monday, still in Hawaii, I had a meeting with some colleagues to decide whether to hold or cancel a PT event. While most of us agreed on a wait-and-see method, one colleague was not happy with the decision and had somehow anticipated or learned of the seriousness of this virus. Only 24 hours later, I would share his opinion that we absolutely had to call off the event (of course now, this is commonsense). In that one day, things had started to fall apart back in Colorado, and I had realized the gravity of what was happening.
All of a sudden, the Govenor was closing down everything in the state. Our county and town had also taken aggressive actions to stop large groups of people from congregating – first no more than 50, then 25, then 10, now 5. From a place of relative comfort in Hawaii where very little was happening COVID-wise, these seemed like drastic measures. Was our Governor OK? Or some kind of germaphobic lunatic?
Because of the craziness in Colorado, we decided to stay a few extra days in Hawaii. There were about 3 extra good beach days in Hawaii before the gravity of COVID-19 hit – then it became time for us to get out. Our flights all started getting cancelled, there were protests to shut down the local airport, quarantines for all arrivals were put in effect. As much as I love Hawaii, I didn’t want to get stuck there. Following many hours on the phone and internet with United and Hawaiian Air, we eventually ended up on a red-eye direct to Denver with a newborn and toddler. We safely made it home in time for me to return to work the next day.
I share this story to say that COVID has an interesting effect of people thinking they’re OK until they aren’t. That original colleague who wanted to cancel our event KNEW already, then the Colorado Governor KNEW, I didn’t know until a full week later. If you’re still out there thinking we don’t need to be social distancing yet, your time is coming. You too will KNOW soon. Please be safe.
Aspen Mountain. Normally people are getting their last slushy turns of the season in and the final mountain parties are happening. Instead, Closed. Shut. Done for the season. Much of the summer activities already cancelled as well.
Running parallel to my timeline in Hawaii, watching Colorado respond from afar, an interesting story was playing out back home in Aspen. A group of Australians had visited and brought COVID with them – even a month later, we only have 30-something confirmed cases in our county, 10 of them are those dang Aussies. Two of these patient-zero-Australians decided to quarantine-in-place at their 5-star slopeside hotel on Aspen Mountain, with the knowledge and agreement of the hotel staff. BUT, they did something no one could have anticipated – those awful, awful people snuck out and went skiing with the general public, putting everyone at risk.
It’s my understanding that their indiscretions is what closed down our city, county, and ultimately the state very early in this pandemic. Those arrogant jerks may just have saved us. Time will tell.
At work, I continue to be gainfully employed – at least as I write this, but nothing is certain. We have trimmed down to “essential” patients only, basically anyone who will be permanently disable if they don’t see a Physical Therapist right now, mostly post-ops. I have about 1-2 patients each day and am managing to stay impressively busy with projects. Administration indicates that they are keeping everyone they possibly can working in whatever capacity they can so that if a “surge” comes, our workforce is immediately ready. Hopefully that surge never comes. I have heard our anticipated peak is April 17th. So, the moment of truth draws near.
Our hospital held onto our travel PTs as long as they could until they finally had to cut them loose this week. In talking with the travelers, no one seemed to be surprised, they were happy to be kept on as long as they were. They were let go with a couple weeks of pay and free housing for a few weeks. It was nice to see the hospital treating the travelers well despite having to make some tough decisions at their expense. Which finally brings us to the point of this post.
This is an awful, awful time for many workers in this country, Physical Therapists included. I don’t have any hard numbers, but casually, it seems like 50% of PTs have been cut from their jobs. If you are a traveler and have had your contract cut short, you are not alone, there are many out there just like you. From what I hear, there are some jobs out there that still have openings, particularly in home health, acute, and SNFs. So don’t forget to open yourself up to the possibility of a new opportunity – just in case you can find one.
If you have suddenly found yourself without a job, I hope your agency or your employer is treating you well to the best of their ability. This time is putting a strain on everyone, and I think we all need to embrace a piece of the sacrifice, employers included. Some clinics will not re-open, many PTs will not return to the clinics that laid them off, PT practice and our society will be forever changed. We are living through a historic event the likes of which very few people have ever seen in their lifetime and hopefully we will not see again. This period in time will go down with the Spanish Flu of 1918, both World Wars, and 9/11 – it’s going to be rough, but it will pass. And some of those events of the past have been defining for our profession.
In talking about Aspen and WWII in the same breath, I must mention the 10th Mountain Division that had its roots in this area. A very fascinating history if you are finding yourself with time to read.
When this is all behind us, people’s knees will still hurt, their backs will still hurt, and they will still suffer strokes and heart attacks. Lots of people will need PT when this is all over! I hope for a very quick rebound, particularly in the realm of clinics needing temporary staffing. When people feel safe coming out of their homes, they will need our services. Hopefully that happens sooner rather than later.
In the Meantime… here are some opportunities to ease the pain.
Emergency License Waivers/PT Compact
There are still some employment opportunities out there. Many hospitals are overwhelmed at this time. It makes sense that as many thousands of people recover from the novel Corona Virus, they will require inpatient rehab needs in a SNF, or the will need home health. If you’re looking for work, it is these setting I would be looking in right now.
I’ve heard some people talking about a possible Federal mandate to open licenses across borders. The main challenge to this happening is that professional licensure is a state protected right by The Constitution. We are far more likely to see more state waivers on licensure like we are seeing emerge now.
The link below from FSBPT is tracking the measures states are taking to allow healthcare workers to come into their state to help in this crisis. There is a huge variation of waivers state-to-state, so your best bet is to click on the link below and see where you might qualify for temporary practice.
A couple examples of what is going on out there:
California – allowing people with inactive and expired CA licenses to re-activate within a matter of days.
Delaware – Allowing graduated, but not licensed PT and PTA students to practice under a licensed clinician.
New Hampshire – Specifically allowing out of state licensed professionals to practice telehealth.
There are a lot of people out there advocating for our role in this global emergency. Our profession evolved to resemble what it is today out of Reconstruction Aides during the first World War and from needs presented during the Polio Epidemic. Our success or failure in responding to this crisis will shape our profession in the future. If we want to be an essential service in the future, we better demonstrate the uniqueness and importance of our skills NOW.
There will be no one else mobilizing and strengthening the thousands of patients who recover from COVID-19 with significant lung damage that needs our skills. All the people that are sitting sedentary at home right now are going to need us badly when they try to leave their homes again. There will be major societal repercussions from this time of solitary confinement. Don’t be mistaken, if you don’t see our essential need yet, you will – it’s coming.
APTA has collaborated with others to develop a volunteer pool matching available professionals and students with needs for volunteers. If you are available, please consider signing up at the link below – while it might be a little scary, this is a great opportunity to be a part of the heroic response and gain some new skills along the way.
There is a tremendous amount of information available for free these days. There are existing resources and new ones that have been recently opened up. If you are finding yourself with extra time to occupy, here are just a handful of ways to expand your mind, but I encourage you to search for more. There’s a ton of stuff out there.
The Academy of Orthopaedic Physical Therapy has release a reading list that was previously a part of a paid course. This reading list is a greatest hits of Orthopaedic Physical Therapy literature and long enough to keep you occupied for months: ow.ly/Z4bT50x2xHT. AOPT has also decreased the price on many of it’s archived courses. You won’t receive official CEUs for these courses, but I’ve taken several of them and they are very meaningful learning opportunities produced by the absolute experts in our field. For $10 or $20 you can get some great education: https://www.orthopt.org/content/education/independent-study-courses/browse-archived-courses
Meditate. Headspace is a online service focusing on guided meditations. Now, they are offering their premium service for free to healthcare workers through 2020. This may be the single most valuable resource on this list. Whether you are under-worked or over-worked, some meditation could probably do you some good in this time. Mental health is so important in a time like this.
Many universities offer free courses on a regular basis including Harvard. I’ve always wanted to check out what they have to offer, now might be that chance.
Audio Books – Audible has over 1,000 titles available for free. With school being out, they have added a whole bunch of children’s books which includes many of the classic. Might be time to review some Mark Twain or Hemingway.
Learn a language. If you are, or live with, a student of any level, both Rosetta Stone and Babbel are offering 3 free months of courses in a lot of languages.
Unemployment
If you have been laid off, furloughed, or have had to step away from work to care for a loved one, you are eligible for unemployment benefits. Who is available has been expanded by Congress and they are supplementing the weekly benefit by up to $600. I’m not so polished on the details, but this APTA page explains some of the details and links to the Department of Labor who is ultimately in charge of implementing the changes.
Congress included the gig-economy and contract workers in this expansion. I have to imagine there are Unemployment Benefits that extend to travelers given those two area of focus. It is also likely further expansions of unemployment will come.
That’s all I have in me for now. I have the intention to write the second piece to examine what positive changes our profession and our society can take from this experience… we’ll see what comes of that as the next couple weeks progress.
This is a grave time, historic in all the worst ways. I hope our profession can pivot to meet this time’s needs and come out stronger on the other side. Stay safe out there. Take care of yourself. Take care of each other. We’re going to get through this, and PTs will be VERY busy in a couple months.
Back in PT school in the early 2000’s, Vision 2020 was recently developed and all the rage. Everywhere I turned, I was hearing about Vision 2020 and the Guide to PT practice.
I’d like to take a look back at Vision 2020, and where we are today in… the year 2020. I’ll admit, this isn’t really fair. APTA’s House of Delegates (for which I am now a Delegate) moved on from the Vision in 2013 with an updated even further forward-looking vision. Also, anyone my vintage of PT and younger grew up with the existence of Vision 2020 and of the Guide – it’s all we’ve ever known. I shouldn’t be evaluating this, it would be far more interesting for someone with just a few years more experience than myself to do this analysis, because they were practicing before these ideas existed. The graduates of the early 2000’s graduated into an extraordinarily transformational time for our profession.
Let’s go at this, one goal at a time.
Autonomous PT Practice
I don’t think any of the other goals exist without autonomy. All of the tenets of Vision 2020 are interwoven, but Autonomous Practice seems to be woven throughout.
Physical Therapists have made great strides towards and in autonomy. In its true meaning, autonomy, indicates that we are making clinical choices for the good of our patients without outside influence. Unfortunately, I think full autonomy is near-impossible. There are always influences external from the needs of our patients. Limitations in resources – time, money, equipment, technology, training – will always limit what we can do with our patients. Add in the further impacts payers and employers have on our practice, and full and complete autonomy begins to look like a pipe dream. However, from the view point of PTs being technicians under Physicians only a few decades ago, we have come very far.
I’d like to highlight 3 areas I personally work in that demonstrate different implications of our progress towards professional autonomy.
This is a travel PT site, right? Well what better way to be autonomous than to work for whoever you want, whenever you want, wherever you want. I believe travel PTs are leaders in the movement of our profession to be autonomous.
It’s easier to be brazen in your beliefs and values when you are only planning on working for an employer for a short time. Stereotypically, travel PTs are often viewed as lazy, or just showing up for a check each day between bouts of play. There may be a segment of travel PTs that embody this negative stereotype, but the majority of travelers I have met are go-getters that aren’t willing to accept the status quo. This is a segment of our profession that is always looking for more – new places, new people, new experiences. More often than TAKING advantage of the system, they tend to GIVE much more to the practices they work in. I have heard story-after-story of travelers working for practices in which they improve patient care and fix incorrect billing practices. Most travelers are leaders in autonomy in that they are not beholden to a single employer. They are able to bring the best of all of their experiences to a single practice – as long as the practice’s managers are willing to listen.
In another part of my life, I’ve recently increased my work in the non-insurance sector. My wife, primarily, and myself set up our own business to bring PT to the people (who are willing to pay cash for our services). Concierge PT Practices are popping up in communities all over America to serve patients directly, but the patient population is not who I thought it might be. Living in a community with an affluent population, I expected my patients to be the millionaires and billionaires. So far, most of my clients are ordinary people who respect the value of great Physical Therapy and are willing to pay for that great care. My brief experience has made me realize that any good PT could set up a mobile practice anywhere. Concierge PT must be the most autonomous practice there is – no boss, no insurance payer, just the clinician and the patient.
Finally, I’d like to discuss my full time day job – PT for a hospital. I find it a little hard to reconcile my desire for autonomy and that not only do I have my PT boss, but then I have his boss – an RN, her boss, her boss’ boss, and eventually a Board of Directors, a couple of whom are Physicians. While I do like all of these people personally, they each create barriers that prevent me from being able to treat my patients the way I should without restrictions. To be fair, they aren’t creating most of the barriers, but they do have the responsibility of enforcing restrictions imposed by payers, bureaucrats, and auditors.
At my full time job, PTs recently started ordering imaging. This is an area of PT practice that I believe is the next frontier. We are well trained in when musculoskeletal imaging is needed – more so than the typical people ordering imaging. I believe you’ll see many more PTs ordering imaging in the next few years.
If I am so vehemently against Physician Owned PT Services, then how do I work for a hospital? How do I sometimes work in that hospital’s Orthopaedists’ office providing care under their purview? Like I said, I can’t fully reconcile these things, but I know this: 1. The care I’m able to provide in this work setting is excellent. 2. My being in the Orthopaedists’ office gets PT to more people earlier than my not being there. 3. Hospitals are a huge piece of our health care delivery system and that’s not going to decrease anytime soon – it is better that PTs are an integrated part of the Medical Model, than to be on the outside looking in.
There is a positive side of autonomy to my working in the hospital – we have a lot of resources and are able to practice at a high level approaching the limits of our scope of practice. We see patients via direct access, we order imaging, and we get to impact patients in a lot of different settings – outpatient, inpatient, emergency, Physicians’ offices. Luckily, I am empowered to use all of my skills. “Autonomous” doesn’t have to mean “independently PT owned”, to me, it simply means practicing the best you can without unnecessary negative influences.
Doctor of Physical Therapy and Lifelong Education
Whelp. We did it! In 2016, the mandate kicked in that all PT education programs must be at the Doctoral level. Of course, all programs had switched over before 2016. Many Masters programs were transitioning when I graduated in 2006, and the very first Doctoral programs cropped up well before that in the late 90’s. We’re more than 20 years into this pursuit of a Doctoring profession, DPTs are quickly becoming the majority – mission accomplished! …or is it?
We have a persistent history to defeat. We are still viewed by many Physicians as technicians, subordinate to them. Many of us DPTs are hesitant to use the word “Doctor” in association with ourselves. Laws have not caught up with our advanced education – we’re still fighting legislative battles hindered by what the education level of a PT was my entire lifetime ago. In contrast, Chiropractors just popped up as “Doctors” one day (at the end of the 19th Century). Although they have had their own tribulations over the years, it is my contention that their unwavering use of the term “Doctor” has granted them many legal wins over the years that we have yet to be afforded. We are still fighting ghosts of what our profession used to be, not what it is today. We were formed under Physicians and the medical model – a history that has great advantages to our profession, but also a history that keeps us down as the underlings.
Another important aspect of being a Doctoring profession is acceptance of the responsibility of being a portal of entry into the health system – meaning we might be the first professional and person with a serious condition sees. We must fully accept responsibility for the care of patients and appropriate referral if needed. This is something that PTs are trained to do routinely these days, but more of us need to be able to articulate exactly what that responsibility is and that we accept it. Too often we rest on the liability of a supervising Physician while crying for the respect of an independent professional. We can do better.
So are we a Doctoring profession? Sure. But to be respected as one, we first all need to embrace our high, high level of education and our rightful titles as Doctors of Physical Therapy (I could go on-and-on about this, and have previously). We need to keep fighting the battles against outdated legislation and seize every opportunity to demonstrate our knowledge and great abilities as THE experts in conservative physical medicine. And, we need to fully accept the responsibilities that come with our rightful position as experts.
Direct Access
We have made great strides in direct access to Physical Therapists. Some form of direct access exists in all 50 states – in every state, people have the legal right to see a Physical Therapist with no prior Physician visit. However, in many states, this is not unrestricted direct access. There continue to be requirements for Physician supervision or approval of care – a complete and total farce. I’m an expert in rehab, I don’t know why I would pretend to supervise the care of a Surgeon, but Surgeons, with little training in rehab, must often certify the work of rehab specialists – a bizarre policy at best. The largest insurer in the country, Medicare, requires Physician certification of the PT Plan of Care. This is perhaps our greatest barrier in achieving unrestricted Direct Access.
There is no reason there should be anything but full and open Direct Access for every Physical Therapist in America. The reason there isn’t is, again, our long history as technicians and underlings to Physicians. Regulation, both in insurance and state law, has not caught up to our current training. The need for a Physician referral for Medicare beneficiaries is completely ludicrous. Far less educated individuals “treat” people with pain all the time without MD supervision – ever heard of a Massage Therapist or Personal Trainer needing a Physician referral? Full and unrestricted direct access will come, but it will take time, and it will continue to take a lot of effort to change existing laws and dogmas. We can not give up the fight, and advancing Direct Access should remain a top legislative priority.
Evidence-based Practice
Oy Vay. What do you say about this.
It is generally accepted that any evidence takes 17 years to fully implement. Our profession’s standard of care will likely become more-and-more evidence based as time passes.
There are factions of our profession that are not evidence-based. Some are using new techniques that are not evidence based, others continue old habits that are dying a slow death. I’m looking at you, Cranio-Sacral. I’m looking at you cranial suture mobilizations. I’m looking at you Ultra Sound.
I am definitely not opposed to innovation. If we, as clinicians, never stepped outside precisely what the research says, there would be no advancement of our techniques. Practice often drives novel research, not necessarily the other way around. Many are trying to standardize care (aka “Decreasing Variance in Practice”), but I think one of our profession’s great strengths is having a certain level of variety in what each of us can offer. If we were all Fellowship-trained Orthopaedic Therapists, our profession’s impact would be across a very narrow population. Instead, we are broad in our strengths, interest, and post-professional training. No matter who a person is, or what their physical ailment is, there is a physical therapist that can meet their physical and psychosocial needs. I think this variety is a strength.
Despite some of our variability, our profession is far more evidence-based than anybody else treating in our domain. Seriously, please write me if you come up with a profession that is treating patients without medication and surgery with a more scientific and comprehensive approach than us. No one is! I can’t think of anyone treating pain and functional impairments with more science than us. That is our area. That is our expertise and no one else’s.
Professionalism
I apologize. I’m going to sweep this one under the rug. Professionalism, I think you got it, or you don’t. Please strive to be professional.
In Vision 2020, professionalism is described as, ” Physical Therapists and Physical Therapist Assistants consistently demonstrate core values by aspiring to and wisely applying principles of altruism, excellence, caring, ethics, respect, communication and accountability, and by working together with other professionals to achieve optimal health and wellness in individuals and communities. “
That’s very aspirational and intangible. I’m going to just move onto the next bullet point.
Practitioner of Choice
Nope. We haven’t done it… YET.
But this goal is a really big deal.
I really hate to bring up Chiropractors again. I don’t mean to pick on them, perhaps they would see my attention as a compliment. In the realm of non-invasive musculoskeletal treatment, they are our biggest competition. Because of our advantage in being more evidence-based and having a broader education, I don’t see how they possibly compete with us once our whole profession has caught up to the level of our current Doctoral education.
Do you know those regional for-sale groups on Facebook? We’ve got one here in our area, and every so often, someone posts something about the injury they have recently suffered asking who they should contact for help. The vast majority of replies for these injuries are to go see particular Chiropractors. I can’t explain it – maybe the type of person replying to online calls for medicine lends itself to advocates of Chiropractic? Regardless, there is a huge percentage of people choosing Acupunturists, Massage Therapists, “Body Workers” (generic term for any person without a state license who wants to touch you), Personal Trainers, Naturopaths, and, yes, Chiropractors.
In research, I’ve seen estimates of <20% of people who have conditions for which PT is indicated actually receive PT services (some estimates as low as 8%). That is a tiny percentage which we must continue to work like crazy to expand. Every effort our profession has, and every individual in the profession, should be working towards expanding the number of people who eventually find a PT for their pains. Outreach and collaboration will be huge in this endeavor.
I’m lucky enough to live in a community where Physical Therapists gained respect a long time before I was here. The regulations of Colorado helped shape the landscape for Physical Therapists to practice at their best (full direct access in the 80’s). A very active local population has consistently provided a population of people injured and looking to avoid surgery. A long-term and close relationship between PTs and local Physicians has developed trust and respect for our profession. These are the things we must try to incubate in every community in the country. We can become the practitioners of choice, there are plenty of potential clients out there, but it will take persistence and lots of work on a micro-local level.
All of the above goals set us up to be the best professionals to treat anything that stands a chance at recovery without surgery or injections. We will never reach a point where every Physician chooses us as a profession to refer to. We will never reach a point where every patient has a Physical Therapist as their first choice for every ache, pain, and limp they have. But, with everything that has changed about Physical Therapy over the past 20 years, we are undoubtedly the best choice, if not the first choice. We’re well on our way, but must keep striving to achieve the goals of Vision 2020.
A couple weeks ago I found myself sitting at a small breakfast table with 2 past Presidents of the American Chiropractic Association (ACA) and some current ACA board members. For anyone who knows me well, this is a very unexpected place to find me – I am acutely aware of and involved in the many legal battles that have taken place between Chiros and PTs over the years. Now that I’ve had some time to reflect on the whole experience meeting with Chiropractors, I’d like to share it.
With the scene set, I must pause for a second and write a little about my writing process. At the beginning of a typical post, I have an idea and I start writing. Sometimes I don’t know where I’ll end up, other times I do, but I never know what the middle of the piece will look like. This time, I know I will end with a message of hope and collaboration between professions that have often been adversaries over a few decades. I only tell you this in order to convince you to read to the end. I can’t imagine I won’t disparage some Chiropractors along the way, it might get ugly – just stick with me, the end is positive.
There’s a local Chiropractor, who as with any other practitioner in a small town, I share some patients. She and I have never really met each other, but we’ve been in the same room enough times that we know who each other are. We share some great friends in common. Because of the people she is friends with, I can’t imagine that she is not a good person – but as a professional…. uhg. Her clients routinely come in believing they have “had Physical Therapy before”. I was shy at first when patients would come in telling me they already had Physical Therapy, but now I plainly reply, “You have not had Physical Therapy. She is a Chiropractor, you have had Chiropractic, not Physical Therapy”.
This single Chiropractor is emblematic of my relationship with the Chiropractic profession over the years.
My introduction to back pain was through an injury I suffered wrestling in high school. I originally went to see a Chiropractor who was the father of a soccer teammate. After my first Chiropractic treatments, I was hooked. Manual Spinal Manipulation feels good… but it didn’t fix what would eventually turn out to be a spondylolysis, a.k.a. decapitated scotty dog, a.k.a. fracture in my L5 spinous process. Chiropractic adjustment felt good, I loved it, but it wasn’t curing my spinal fracture. I eventually would wear a lumbar brace for 9 months, take some less-than-recommended time off sports, and get a short course of Physical Therapy that I hardly remember.
Fast forward several years, and I’m at Northeastern University in a pre-PT program bringing in Chiropractors to talk to our class so we can understand their profession, as well as ours. I was that guy. I was the guy who brought Chiropractors into school so we can all learn from each other and practice in a happy collaborative world of bliss.
Chiropractors ruined my positive attitude about them – there is no one to blame but them. I got involved in APTA in Massachusetts, then the states I lived in as a travel PT, and then nationally. One constant persisted across my experience – Chiropractors suing PTs across the country over pointless turf battles. The lawsuits centered mainly around two topics, PTs performing manipulations and PT Direct Access (without a Physician or Chiropractic referral). These lawsuits were not based on patient safety, they were only based on a perceived threat to Chiropractors’ bottom-line. These lawsuits developed a long, dense history of contention between the two professions that eventually led to last month’s Interprofessional Collaborative Spine Conference (ICSC) to start healing some wounds.
The ICSC brought together PTs, Chiropractors, and Osteopaths to discuss manual spine treatments.
The structure for the conference was essentially this: For two days, panelists presented topics, then opened up to audience questions for further discussion. The presenters and audience were largely leaders in PT and Chiropractic, (and Osteopathy). The questions were engaging and on-point – the presenters were the best-of-the-best in our fields. There was zero contentious discussion that was had. In fact, I found the formal content of the conference pretty underwhelming.
The good news is, there was a lot of time scheduled for social interaction and networking. This is how I found myself having breakfast with Chiropractic’s heavy hitters. The very individuals I have grown accustomed to battling against in state legislation over-and-over again, I was having a polite breakfast with, exchanging stories of insurance interference in our practices, and exchanging business cards. I think I behaved myself, and the conversations were enlightening for me.
The time in between the sessions was invaluable for me. It allowed for open, cordial conversation about a variety of topics. We talked about our education, our practice, our research training, and our common interests. It added to my understanding of the loooong histories that make the Physical Therapists, Chiropractors, and Osteopaths what they are today. Our current-day practices are deeply entrenched in the histories of our professional origins over the last 100 years and long before.
After digesting the conference for a couple weeks, I now more strongly than ever believe that the Physical Therapists have the higher ground on whose practice is more evidence-based. I hope that the Chiros and DO’s walked away saying to themselves, “Whoa, did you hear that content from the PT presenters?” That was definitely my reaction. But, more likely than not, their reaction, like mine, was something reinforcing their own practice beliefs. But, maybe they are onto something too. Chiropractors have a very effective model in making people feel good (if only for a little while). They don’t allow themselves to feel overly limited in doing exactly what the science dictates, they just manipulate and know it makes a lot of people feel good. They do have a point.
I could go on. And on. And on about how I believe PT is more superior in research based practice, that’s our training… but that’s not the point. They clearly have something good going on with the way they practice too. We will not align Physical Therapist and Chiropractic practices for a very long time – our histories are too different.
There was a great common thread of conversation that reflects the impetus for this conference. Research does, indisputably show, that patient interaction with a Physical Therapist, a Chiropractor, or an Osteopath decreases prescription medications, imaging, surgery, and, most importantly, cost. One phrase I heard in conversation at the ICSC that has continued to run through my head is, “A rising tide lifts all ships.” So true. Despite our different individual histories, and our many battles against each other, if we can unite to improve access to manual therapists before surgeons, we will save our patients from pain and from the cost of undue medications, radiographs, and surgeries.
I have learned that everything we think we have different with Chiropractors is justified. But we have one major thing in common – either of our treatments decreases more invasive and expensive alternatives. That is something worth burying the hatchet and uniting over.
I wrote earlier this year about some injuries sustained in the Spencer household and our plans to manage them conservatively, at least without immediate surgery. The original piece is here: Doubling Down on Non-surgical Conservative Care.
In a short period of time last winter, Kate had sustained a knee injury and I had a mallet thumb injury (extensor pollicis longus rupture). If we had sought formal medical consultation, surgery most certainly would have been recommended for each. In fact, for my thumb injury, I did casually consult an Orthopedic surgeon who did recommend surgery. I work closely with and respect this surgeon greatly. He did a sort of magic trick – before asking me what happened, he took a look at my x-ray and said, “You can’t extend your thumb, can you?” Magic. Impressive. Brilliant Doctor. But, I ignored his advice, “You’ll likely do better with surgery than without. If it were my thumb, I’d have the surgery.” The contention was that the tediousness and fragility of daily splinting routine sometimes leads to failure with conservative management. The surgical procedure would not repair the torn extensor tendon, but it would better immobilize the thumb so that healing could occur in a more predictable fashion than with bracing. After reviewing the available literature, which was mostly case studies, I decided to take my chances and go with the daily splinting. My expectation was that I would regain much of my thumb DIP extension, but likely come up 10 to 20 degrees short of full extension.
Here I am pressing my thumb into the counter to keep it extended while I work to re-tape and support it. I had to keep it extended on a surface while I washed it, dried it, and taped it daily.
8 weeks of splinting my thumb in hyperextension – untaping, washing, drying, and retaping every morning while passively maintaining extension. After all the splinting, it took another few months of recovery to regain motion and strength. Eventually, my results ended up being better than you’re supposed to get following a rupture of the EPL. There’s a little lag in extension, but I am able to actively hyperextend the thumb. I’ve come away with two conclusions about the conservative management of a mallet injury (thumb or finger) through my reading and through my personal experience:
Early intervention is essential for successful conservative management. My OT co-workers had me splinted within 12 hours of the initial injury – research also indicates that success falls off after only 1 to 2 days if splinting is not initiated.
Compliance, man. Compliance. A person with a mallet injury has to be fastidious about keeping the thumb extended while changing the bandages and occasionally cleaning the thumb. The rule is that if you accidentally bend the thumb, your 8 weeks of splinting starts over – I would contend that each time the thumb is accidentally bent, several degrees of active extension is lost forever. I have myself as a PT, my wife as a PT, and OTs/Certifed Hand Therapists as close friends… I figured I was a good candidate for being able to manufacture 8 weeks of compliance. For our patients, we need to educated them to a great extent on the importance of maintaining extension.
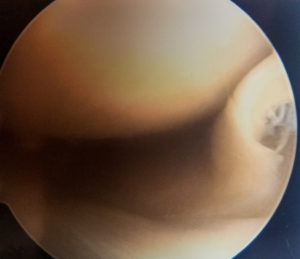
Here, on the far right side of the picture, is Kate’s flipped over bucket handle tear of her meniscus… see it?
Now, Kate’s story is a far more fascinating story that perhaps raises more questions than it gives answers to. While pregnant, she had sustained what I am convinced was an ACL injury. She was super-lax when I tested her Lachman’s on the day of the injury – a very, very late endfeel, lots of translation. Because she had her ACL previously reconstructed, I had actually tested her knee before the injury and knew the knee to be very stable. Because she was pregnant at the time of the injury, she made the decision to wait and see what the knee was like after pregnancy and after the hormones that goes along with pregnancy had passed. After she had the baby, she got an MRI to see what might be going on in her knee since it was feeling much better, but not perfect. The MRI showed some lateral meniscus damage and an ACL that existed but didn’t appear robust. The same Ortho that I saw for my thumb took a casual look at her MRI and commented that the posterior lateral corner damage may be a sign that “an anterior subluxing event may have occurred,” again, great info discerned from what could be interpreted as a fairly benign MRI. Anyways, by this point, the knee was testing more stable and never, ever giving Kate a feeling of giving out. The decision was made to continue with strengthening and conservative management. Over time, the knee felt well on a day-to-day basis. We hiked a fair amount this summer and Kate even got one late-November ski day in without any issue. Her knee was feeling pretty good… until she knelt down two weeks ago. Her knee swelled up and became an immediate problem. She continued to not have any feeling that her knee was giving out, but now it was stiff, swollen, and sore. After pushing through a race 3,000 ft up Aspen Mountain on the injured knee and with the end of the deductible year fast-approaching, Kate and Tom Pevny, an Orthopedist at Aspen Valley Hospital where we work, decided that scoping the meniscus and laying some eyes on the actual condition of the ACL seemed like a prudent plan. Though Kate still had some reservations going into the surgery about whether she really needed it, the surgery was justified when Dr. Pevny let her know that he had taken out a sizeable bucket-handle tear from the lateral meniscus. Had she left it alone, it certainly would have continued to give her troubles.
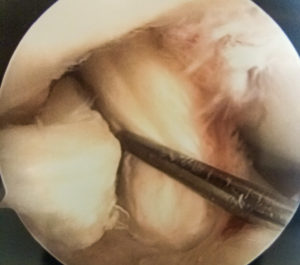
Here is Kate’s intact and robust ACL.
Now for the million dollar question: What about the ACL? Dr. Pevny says it looks good. The stability is that “of a typical reconstructed ACL”. Whenever Dr. Pevny does talks on the ACL, he emphasizes techniques that mimic replication of the anatomical footprint of the ACL and the ability of a well-performed reconstruction to stabilize the knee in various positions – this point is emphasized in his research papers as well. I get the impression that he believes Kate’s previous reconstruction to be adequate but not equivalent to what could be done today. I, on the other hand, believe that Kate’s reconstruction in ’94 was done extremely well, and that the knee was extraordinarily stable with a very tight ACL. I also believe that the ACL was stretched and loosened during her accident last winter. If this is true, that her ACL acquired some laxity, but within an acceptable range that still allows full function, I have a lot of questions that I don’t think current research answers. Did the presence of the hormone relaxin during Kate’s pregnancy actually allow her enough ligamentous laxity to avoid more a serious injury? Did the ACL remain stretched and then “reduce” more than it normally would have when the pregnancy hormones retreated? Does relaxin even act on a reconstructed ACL like it does on a native ligament? I would think it does. There’s a whole string of unanswerable questions that I find just fascinating. If you have any thoughts on my hypothesis and questions, or questions of your own, I’d love you to comment below…
So, in the end: a. My thumb is back to 98% of it’s original self through non-surgical care. b. Kate didn’t wholly avoid surgery, but her patience in waiting to see what the knee did following injury may have allowed her to avoid a long, protracted ACL recovery in exchange for a much quicker meniscal clean-up.
We, Physical Therapists and Occupational Therapists, are THE specialists in conservative management of orthopedic conditions. In circumstances where surgeons and patients are often far too trigger-happy to start cutting, we have to be the balancing voice that educates our clients on the benefits that a little patience and work may have on avoiding surgery which is and should always be the last resort.
I have recently heard a lot about “physical therapy’s identity crisis”. That phrase, “identity crisis,” is uttered by those I know personally, by other leaders in the profession, and by PTs across the interweb. Collectively, we have labelled ourselves as having no consensus on what our role in health, wellness, and prevention. There’s in-fighting about the superiority of treatments centering on pain theory, manual therapy, movement science, and other guru-isms that insist, of course, their way is the best way. But, I don’t think we have an identity crisis. We firmly know who we are and what we do – we may have varied methods of treating our clients, but we do have a central, shared focus. I personally believe our percieved identity crisis has everything to do with a large part of our profession not owning their level of expertise, being shy to demonstrate their full expertise to patients and colleagues, and as cliche as it is, not “being the change”.
10 years ago, we were a profession in flux. I was graduating with my Master’s degree from Northeastern University and almost immediately re-enrolled for my transitional Doctorate, because that’s where the profession was headed. Since the 90’s, things have moved very quickly for our profession from a role as a technician, carrying out Doctor’s orders, to an autonomous profession evaluating patients and safely dictating our own treatments. In a span of about 20 years, universities have propelled us from a 4 year undergrad education to a point where all PT students are trained as DPTs. This relatively quick transition from a 4 year education to a 7 year education did leave us poorly defined for a period, because our knowledge and role did change over that time. Now, it’s about time we get over it. As a profession, we are not at all confused about who we are anymore. APTA’s branding project has been proclaiming since 2009 that we are the human movement experts. The Guide and Vision 2020 had earlier defined what it is we do on a daily basis with our patients and clients. No matter your practice setting or population, human movement is central to your practice – occupational health, sports medicine, acute rehab – even in the realm of cardiopulm, the human body’s ability to move blood and air are central to care. There are some specializations and niches in PT that start to stray from the precise phrase “human movement” – i.e. wound care or veterinary care – but human movement is truly at the core of what the vast majority of Physical Therapists do at work on a daily basis.
So we have had a defined identity for the better part of a decade, why do patients continue to come into the clinic surprised at our education level? Because as individuals, not as a profession, we have refused to embrace the DPT and everything it stands for. I know that somewhere, right now, there’s a private practice owner griping about a patient who has come in expecting to get a massage. This weekend, that same private practice owner will go to a 5K race and give simple, boring, unskilled massages! This is the kind of thing that kills us. Stop giving massages at road races – why not offer gait analyses instead? Or offer mini-consults for ongoing injuries, which there are plenty of in the 5K community. Injury prevention, nutrition, running gear, pain – these are all topics we can consult on with authority. If you give massages at a race, then that is the snapshot of your practice that you are displaying to your community, and people will continue showing up at your door expecting nothing more than a massage. I’m sure you can get more creative with what your practice can do to engage your own community than I can, but please, stop giving massages at races – that’s not Physical Therapy!
We need to be shouting our knowledge from the mountain tops in all of our own communities. Get interviewed on local access cable about injury prevention, write letters to your local and not-so-local papers every chance you get, throw a fit every time physical therapy is forgotten on a TV show, radio program, or news article when we are the experts that should be leading the conversations on musculoskeletal health, not an afterthought. Get verbal, show off your knowledge. Participate in community planning to advocate for healthy and accessible community planning. Even as a traveling PT who is only in communities for a short time, I have hopped on local cable, written letters to local papers, and encouraged others in the community to contact their congressional representatives on topics that matter. It doesn’t take a whole lot of effort to positively and productively promote PT in your community.
Why are we so scared to call ourselves Doctors? I don’t know, but I’m as guilty as anyone else of shying away from routinely using my earned title. We really, really need to embrace “Doctor”, we have each earned it. The Chiro’s sure don’t shy away from the term, and we’re a lot more qualified in providung safe musculoskeletal care than they are. Ever thought twice before calling your Psychologist, Optometrist, or Dentist “Doctor”? These are all non-MD clinical Doctorates – the same as the DPT. In education, even High School, teachers with a Doctoral degree are called Doctor. I really don’t know what our problem is, but we each individually, and collectively, need to get over our phobia and embrace our advanced level of education that matches and surpasses plenty of other professionals who have no qualms with being called Doctor.
Stop looking to leadership for answers on what our role is. Stop looking to APTA to make that one Suberbowl ad that will change the world’s knowledge of PT – that’s not how this works. It’s time more individual clinicians embrace the unique and unmatched work they do in the clinic everyday and demonstrate it to their external community. There are many communities across the country where people do think of their Physical Therapist first when they have an injury. If you think we have an identity crisis, it’s time you changed your identity in your own community. That’s how this works.
Even the restroom lego characters are thinking #NoPolo.
I just finished packing my bag to head off to Nashville for the American Physical Therapy Association’s House of Delegates meeting. To quickly sum up what that is for those of you who might not know: about 500 PTs and PTAs representing different areas of the country, clinical specialties, and/or other interests get together for 4 days to make big decisions about big ideas that will drive the future of the APTA and ultimately the practice of physical therapy. When people talk about APTA doing or deciding this or that, that’s us, this week, and the PTs, PTAs, and Students that attend are all volunteering their time away from their daily jobs. As I pack my two suits and shiny black shoes into my suitcase for the upcoming meetings, I notice how much they stand out in contrast to the rest of the wardrobe I have here in rural Hawaii. I have scrounged together enough black mid-ankle cotton sports socks to get through the week of meetings – I hope they’ll come high enough to gel with the suits. The most dressed up I’ve gotten in the last month is the polo shirt I put on daily to go to work (Is the #NoPolo crowd throwing a fit right now? More on this later.) Each Friday, I throw on an Aloha shirt for an even more formal Friday – here, in this local culture, an Aloha shirt is considered dressing up. The main Hospitalist wears an Aloha shirt every day. The Vice President of the Hospital wears an Aloha shirt every day. As an average Caucasian male, I’m already in the minority here. If I were to show up in anything more dressy than an Aloha shirt or polo, I would be a serious outsider. Dressing in a shirt and tie would, without doubt, affect my ability to connect with my coworkers and my patients. The culture I was raised in has no bearing on the social norms here and formal wear is inappropriate.
On my very first PT job in 2006, a job I took in a private practice that I had done a clinical with, we looked good. Just 3 guys from Boston practicing PT in the farm fields of Vermont wearing button down shirts and nice ties. Aside from our dress, we were goof-balls. Our staff had some really good chemistry there. We were always rambling on about anything and everything to keep our patients entertained and enjoying their time at the clinic. The schtick was constant and super-funny – “the PT will cost ya, the show’s for free.” In that clinic, not too far from Boston and not too far from New York City, we felt great in our shirts and ties, and it was the right thing for the right place – it did, indeed, take our appearance up a notch and add some professionalism to our otherwise juvenile behavior. But, when I left that practice 6 months later for the vast world of traveling PT which would lead to 10 years on the road, I realized that one size does not fit all, there’s more than one way to skin a cat, and, most importantly, rehab can be done best a lot of different ways.
I’ve got a couple patients here from outrigger-canoe-related-injuries. I finally took this canoe (the Kula’ela’e) out with 5 other paddlers the other day. It gave me a whole new appreciation for the biomechanics of the sport. Most kids here grow up with paddling as a part of their upbringing. “Doing is knowledge” in both biomechanics and culture. Whoa, deep.
Later on, Colorado would become my home base, but I still continue traveling out of state on contracts most summers. Several years ago, we had word coming down from the top of the hospital that each department would need to decide on a uniform – I believe this stemmed from a JCO initiative for patients being able to more easily identify who is coming and going from their rooms. I advocated that the rehab department dress more formally – button downs, nice slacks, perhaps ties for the gentlemen. But, this is a mountain town we’re talking about. A place where the wild west is still alive and well. I have seen surgeons make inpatient visits in bike shorts, there’s an anesthesiologist that occasionally roams the halls wearing a cowboy hat, people do not care what you are wearing, they just want the best care from someone who understands their activities and lifestyle. Colorado mountain towns are full of aggro weekend warriors – nay, not weekend warriors, they have come to the mountains to make a lifestyle of outdoor sport and activity – for this reason, the mountains of Colorado respect and understand the role of PTs more than anywhere else I have ever worked. A PT referral is always the first line of defense for all the patients that want the most direct line to getting back out in the mountains and doing what they love. Ultimately the dress code decision was made, there would be no formal dress, the final decision had been made made – black scrub bottoms, white tops, grey (sporty) vest.
I don’t know how I ended up in this place in this blog post. Polos, ties, and sporty vests have nothing to do with the point I’m tying to make. What I’m trying to get at is that things we may accept as simple, given standards in our world may be very different from those held by someone else. I’ve written about local culture before and the great differences geographically in what the norm is, but I’ve been thinking of culture differently lately as I find myself living in more and more rural places. We so often are all encompassing in what we say – when someone says “the world works like this……”, they typically only know about their own experiences. People are so focused on their own world, that they can’t open up their minds and think about how someone lives their life in a community that has less resources, or that is isolated from all major cities, or that doesn’t want their community to be developed into something bigger and shinier. We are all so different from town to town, city to city, state to state, and especially internationally. We often think our own way is the best way, but the truth is that people are so different across our country because of their individual environments, experiences, and upbringings that we are all destined to value different things than our neighbors. We have a lot in common as well, but it’s the differences that can be divisive. I don’t mean to single out the crowd that thinks we should all dress up for work to make ourselves stand out as the autonomous practitioners that we are (I used to be firmly in that camp), but it is just one example that I can grasp tangibly to say dress standards can vary greatly place-to-place, culture-to-culture.
A few of my Aloha Shirts. Flowers and tikis are culturally appropriate. The Red Sox Aloha Shirt is not culturally appropriate unless you are dressing up as two-time World Series Winner Shane Victorino, “The Flyin’ Hawaiian”.
Another area that I have been thinking about culture in recently is research. You hardly ever read an article that breaks down the differences in effect of an intervention on subjects by cultural differences. In research, you frequently read something like, “this study was performed on subjects without confounding past medical histories and the results cannot be generalized to all patient groups.” Why don’t we see cautions like, “this study was performed primarily on New England Suburbanites and cannot be generalized to people of varied backgrounds.” I’m having a little fun here, but I’m serious about the message – people are different and interpret the treatment we administer unto them differently. We cannot hold everyone to our own personal standards and should not expect everyone to have the same values that we do.
I hope that as therapists, we consider the widely varied backgrounds of our patients and that we respect our patients when our best practice patterns don’t align with their priorities. I hope as hundreds of us gather this week to discuss the PT profession that we can open our minds to see how different ways of practicing PT can all be successful for the people who are receiving the treatment and to embrace that difference. Finally, I hope in the greater scope of life that we don’t see people with different political and world views as lesser than ourselves and acknowledge that they merely come from a different set of life experiences.
Travel safe if you are headed to Nashville for the big meeting, I look forward to disagreeing with you all when we get there from our very different places. (just kidding, gosh don’t be so serious)
This website is about being a traveling therapist, right? Then, why so often, do I get myself off-topic blogging and twittering about issues in PT and healthcare? Answer: Because I like it. Only once in a long while do the stars of the interweb align so that I can write about travel therapy and healthcare issues at the same time.
We call ourselves travelers. Traveling therapists, traveling nurses, travel PT or OT assistants – we are all “travelers”. But not MD’s, they, call themselves locum tenens, or just locum for short. Locum!? What the heck does that mean? locum tenens; locum – place, tenens – to hold; all together now, “Place holder”. Turns out locum tenens is actually a Medicare term that applies to someone temporarily filling in for another provider. When someone qualifies to work as a locum, they are able to skip a lengthy credentialing process to be able to bill Medicare patients. The list of providers that are currently eligible for locum status during temporary employment include Physicians, Dentists, Certified Registered Nurse Anesthetists (CRNAs), Nurse Practitioners (NPs) and Physician Assistants (PAs).
There is a Medicare bill currently working its way through congress that would extend locum tenens status to Physical Therapists in certain situations. Currently, in PT private practices, if a temporary therapist is brought in, it can take 3 months to be able to bill to Medicare under their own NPI. Most private practices doing their billing above board and truly the “right” way avoid travelers for this reason. I’m not sure what happens when a private practice hires a therapist through an agency – what I believe happens, is that the private practice bills under one therapist’s NPI. The practice of billing for an entire practice under one NPI, as far as I am aware, is frowned upon, but not illegal. I have done a couple independent contracts with private practices who have made me become in-network at their facility with Medicare, it’s a long process (2-3 months), mostly paperwork, and discourages a lot of employers from getting involved with short-term staff. This bill could change the whole arrangement.
Forget how this whole bill to law thing works? Click above and return to being as smart as you were in middle school.
This new Medicare/locum tenens bill, titled the Prevent Interruptions in Physical Therapy Act (House bill: H.R. 556 and Senate bill: S. 313) would create some exceptions for certain PT private practices. The bill, if passed, would decrease interruptions in patient care that may occur through a PT’s temporary absence due to illness, pregnancy, vacation, or for continuing ed by allowing practices to hire PTs on a locum tenens basis. That would cut out the whole Medicare credentialing process that currently takes place when hiring a temporary PT. While this bill is certainly patient-centric, I do see a secondary opportunity here for travelers. If there’s a current process that inhibits some clinics from taking on travelers (Medicare credentialing), and that process is eased, there’s a lot of opportunity for an increase in the number of available travel assignments. As this bill stands in the Senate, locum tenens status would only be allowed in areas designated as non-Metropolitan Statistical Areas, or areas designated as Medically Underserved Areas (MUAs) and/or Health Professions Shortage Areas (HPSAs) – that’s a lot of private practice clinics that could soon hire temporary employees with less fuss when billing through Medicare. Ideally, the bill would be amended to include ALL areas in the country, not just those of special designation – that would be pretty sick. (it’s a Medical pun, get it?) Be sure to let your Senators know that ALL Medicare beneficiaries deserve uninterrupted access to PT, not just those in underserved areas.
All traveling PTs, everyone in private practice, and all recruiters should be pretty psyched about this bill and should definitely be contacting their Congress Men and Women today. Jump over to APTA’s website to get more information on the bill. From there, you can link straight on over to contact your Senators and Representatives. Get on it now!
SLPs and OTs, don’t worry, I haven’t forgotten about you. If the legislative bug gets you revved up, you have good resources to contact the people who represent you in congress. For OTs: http://capwiz.com/aota/home/ and for SLPs: http://takeaction.asha.org/
I do get fired up about issues, and this one is more special to travelers than most issues are. It was too good not to write about, but I realize healthcare politics can get a little dry. I promise more excitement in my next post!














 I have recently heard a lot about “physical therapy’s identity crisis”. That phrase, “identity crisis,” is uttered by those I know personally, by other leaders in the profession, and by PTs across the interweb. Collectively, we have labelled ourselves as having no consensus on what our role in health, wellness, and prevention. There’s in-fighting about the superiority of treatments centering on pain theory, manual therapy, movement science, and other guru-isms that insist, of course, their way is the best way. But, I don’t think we have an identity crisis. We firmly know who we are and what we do – we may have varied methods of treating our clients, but we do have a central, shared focus. I personally believe our percieved identity crisis has everything to do with a large part of our profession not owning their level of expertise, being shy to demonstrate their full expertise to patients and colleagues, and as cliche as it is, not “being the change”.
I have recently heard a lot about “physical therapy’s identity crisis”. That phrase, “identity crisis,” is uttered by those I know personally, by other leaders in the profession, and by PTs across the interweb. Collectively, we have labelled ourselves as having no consensus on what our role in health, wellness, and prevention. There’s in-fighting about the superiority of treatments centering on pain theory, manual therapy, movement science, and other guru-isms that insist, of course, their way is the best way. But, I don’t think we have an identity crisis. We firmly know who we are and what we do – we may have varied methods of treating our clients, but we do have a central, shared focus. I personally believe our percieved identity crisis has everything to do with a large part of our profession not owning their level of expertise, being shy to demonstrate their full expertise to patients and colleagues, and as cliche as it is, not “being the change”.